Insomnia Treatment: From CBT-I to Medication Decisions

One of the most important elements for human health is sleep, and yet there are millions of people around the world unable to get the quantity of sleep they require. In Australia, now the focus of our series, one in three adults is thought to suffer from some sort of insomnia treatment. There’s no question that losing a little sleep is a common occurrence, but long-term insomnia can cause serious harm to your mental, emotional, and physical health.
When insomnia becomes chronic, interventions such as Cognitive Behavioral Therapy for Insomnia (CBT-I) are generally the first line of treatment. But what do you do when CBT-I fails to alleviate symptoms completely? When should I think about using medication? This story traces the path from CBT-I to insomnia medication, giving readers the knowledge to decide on their options.
What is Insomnia?
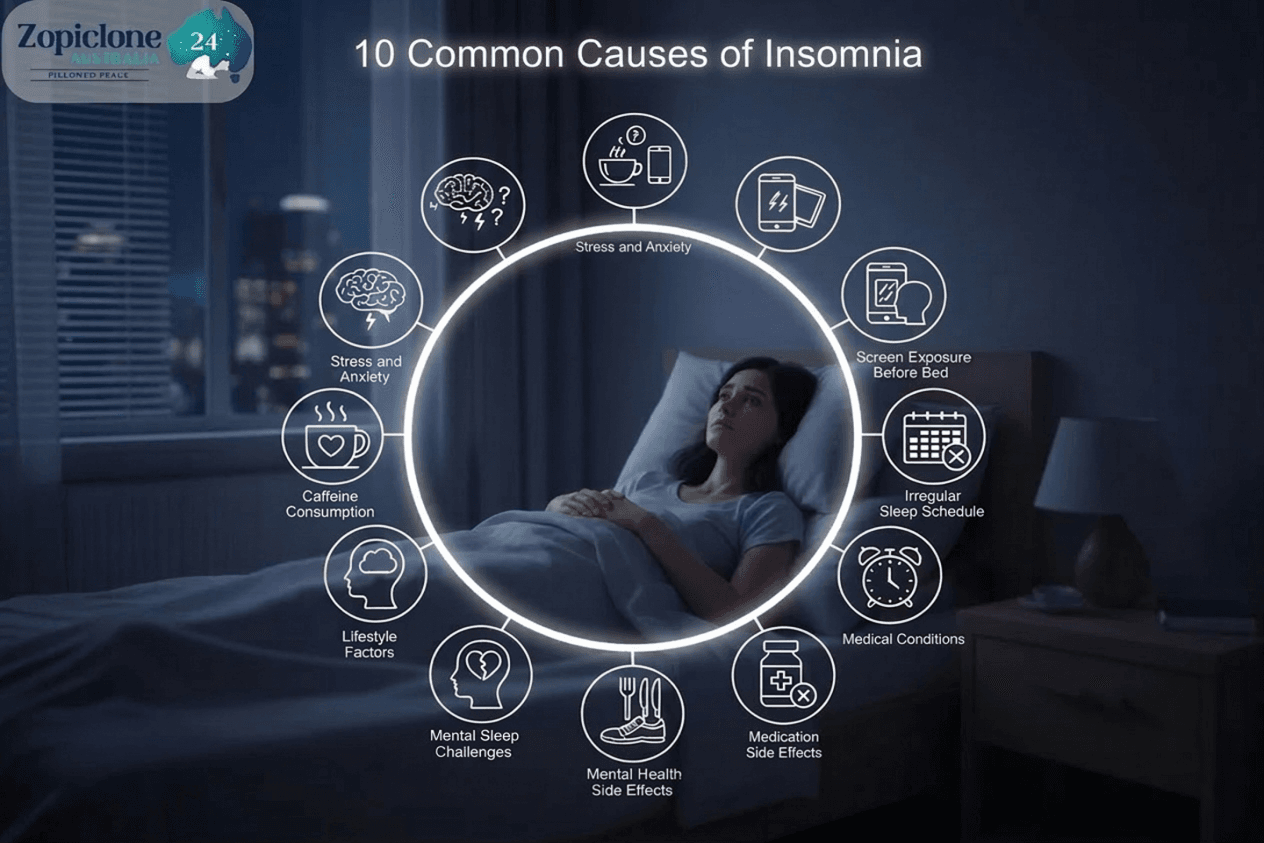
Insomnia is a sleep disorder, and is defined as difficulty falling asleep, or staying asleep or waking up too early and not being able to fall to sleep again. It can lead to day-time sleepiness, irritability, impaired concentration, and reduced quality of life.
Insomnia can be classified as:
- Acute (short-term) insomnia — This type of insomnia is brief and lasts a few days up to several weeks.
- Chronic (long-term): Happens at least three nights a week for three months or more.
Why Is Treating Insomnia Important?
Left untreated, chronic insomnia can contribute to a host of problems:
- Increased risk of anxiety and depression
- High blood pressure and heart disease
- Impaired immune function
- Poor cognitive performance
- Reduced productivity and quality of life
Effective treatment is essential not only for sleep improvement but for overall health.
CBT-I: The First-Line Insomnia Treatment
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the accepted gold-standard intervention for chronic insomnia. CBT-I is recommended by Australian and international sleep specialists, GPs and psychiatry professionals and targets the psychological and behavioural aspects of insomnia.
Key components of CBT-I include:
- Cognitive restructuring: Challenging negative thoughts about sleep.
- Stimulus control: Relearning to associate bed with sleep, not wakefulness.
- Sleep restriction therapy: Limiting time in bed to increase sleep efficiency.
- Relaxation techniques: Breathing exercises, mindfulness, and progressive muscle relaxation.
- Sleep hygiene education: Improving bedtime routines and sleep environments.
Effectiveness:
Research indicates that when patients are committed to it, CBT-I can produce a substantial and enduring improvement in sleep onset, quality and duration — without many of the dangers of side effects that accompany medications.
When CBT-I May Not Be Enough
While CBT-I has been an effective treatment, it doesn’t help everyone or in every situation. Some people may not have access to qualified therapists, or they may not have the time or inclination for group or individual therapy, or they may have accompanying problems that render CBT-I less effective by itself.
Situations where CBT-I might fall short:
- Severe, treatment-resistant insomnia
- Co-occurring mental health disorders (anxiety, depression, PTSD)
- Insomnia secondary to chronic pain or serious medical conditions
- Urgent need for short-term sleep improvement (e.g., extreme stress, bereavement)
In these cases, physicians could advise the inclusion of medication as a second line option.
Also read: How Long Does Gastro Last? Symptoms & Recovery Time
Medications for Insomnia: When and Why
Pharmacological treatment of insomnia Ideally medication should be prescribed after CBT-I, or as an adjunct to it, if patients continue to experience symptoms. Symptom relief can be achieved with short-term pharmacologic treatment, especially during crisis situations or while waiting for the benefits of therapy.
Common reasons for prescribing sleep medications:
- Immediate relief from severe insomnia
- Managing insomnia during major life stressors
- Situational insomnia with clear, temporary triggers
- Enhancing CBT-I’s effectiveness in some cases
Types of Medications Used for Insomnia
- Benzodiazepines (e.g. temazepam)
Traditionally used for short-term insomnia but carry risks of dependency and tolerance. - Non-benzodiazepine hypnotics (e.g. zopiclone, zolpidem)
Fast-acting medications effective for sleep initiation, considered safer than older benzodiazepines but still recommended for short-term use. - Melatonin receptor agonists (e.g. melatonin supplements)
Helpful for circadian rhythm disorders or mild insomnia, especially in older adults. - Sedating antidepressants (e.g. mirtazapine, amitriptyline)
Often used when insomnia co-exists with depression or anxiety. - Over-the-counter options
Antihistamines or herbal sleep aids may offer mild relief, though evidence of efficacy is limited.
Note:
In Australia, prescription drugs including zopiclone need an evaluation by a doctor. It is generally important to use these medications with medical oversight to prevent dependency and unwanted side effects.
Balancing Benefits and Risks of Sleep Medications
These drugs can work very well, but their use is generally limited to short-term or on-an-off-basis due to disadvantages:
- Risk of tolerance and dependence
- Daytime drowsiness and cognitive impairment
- Interaction with other medications
- Rebound insomnia upon discontinuation
Healthcare professionals balance these risks with the benefits when prescribing medicines: some of which may or may not be alternatives to NSAIDs and which include taking the lowest effective dose for the shortest period necessary.
Shared Decision-Making: Choosing the Right Approach
The decision regarding when to transition from CBT-I to medication is one that should be made jointly by the patient and clinician. It involves:
- Comprehensive evaluation of insomnia’s severity, duration, and impact
- Assessing underlying medical or psychiatric conditions
- Reviewing previous treatment attempts
- Discussing the risks and benefits of medication options
- Setting clear goals and timelines for medication use
The Ideal Treatment Plan: Combining CBT-I and Medications
In certain cases, a combination of CBT-I and medication is more effective than either therapy alone. For example:
- Short-term zopiclone treatment to normalise sleep patterns while other CBT-I strategy is being pursued
- Melatonin supplements in combination with sleep restriction therapy
- The use of medication at the time of an acute insomnia episode, with ongoing CBT-I for the longer term deferiprone.co.uk.
This comprehensive method provides a means of treating both the presenting symptoms and the underlying behavioural and cognitive causes of sleep disturbance.
Accessing Insomnia Treatment in Australia
For those seeking help in managing insomnia in Australia:
- GPs: Initial assessment and referral point.
- Sleep specialists: For complicated or stubborn cases.
- CBT-I trained psychologists: Can be accessed via private practices or mental health plans.
- Online CBT-I programs: Evidence-based programs such as This Way Up or Sleepio remotely provide therapy tools.
Sleeping remedies include zopiclone, either in 7.5 mg or 10 mg tablets prescribed on a short term basis after clinical assessment.
Our Product: Zopiclone/Zopfresh 20mg Tablets
Final Thoughts
Insomnia is tough. But there are many ways to treat it. But though CBT-I continues to be the first-line prescription for chronic insomnia, there are occasions on which medication can be beneficial — especially in more severe or resistant cases.
Personalized care, consideration of the risks and benefits, and involvement of the patient in treatment decisions is the key for an optimal management of insomnia.
| Field | Information |
|---|---|
| Written By | Dr. Michael Anderson |
| Checked By | Dr. Daniel Thompson |
| Published Date | 5 May 2025 |
| Next Reviewed | January 2026 |
| Category | Sleep Disorder Treatment |